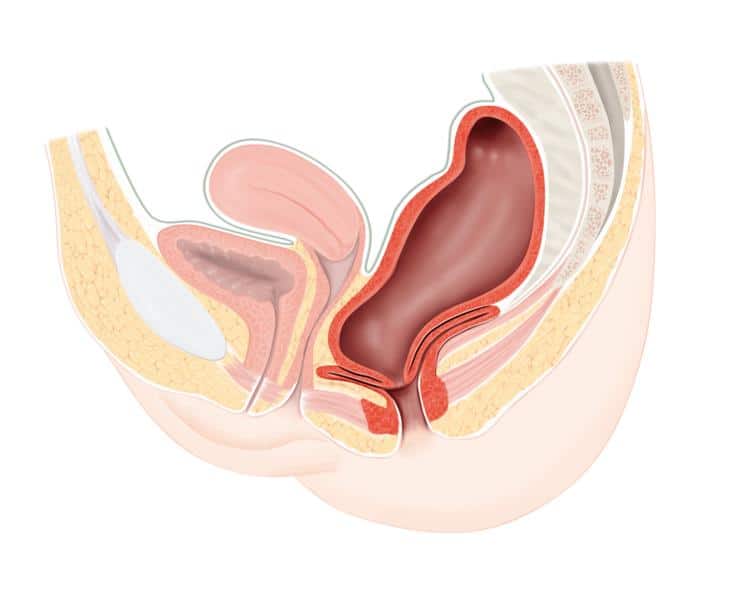
Obstructed defecation syndrome, severe constipation, rectocele (rectum bulges into vagina)
Obstipation is a common symptom that can be divided into slow transit and outlet obstruction, which is discussed here. The frequency of defecation comprises a large spectrum from 3 times a day to once every 3 days if a person feels good without any complaints. Further examinations are necessary if one or more criteria of the obstructed defecation syndrome (according to the ODS assessment score) are prevalent, e.g., bearing down, sensation of incomplete defecation or rectal blockage or manual support during defecation.