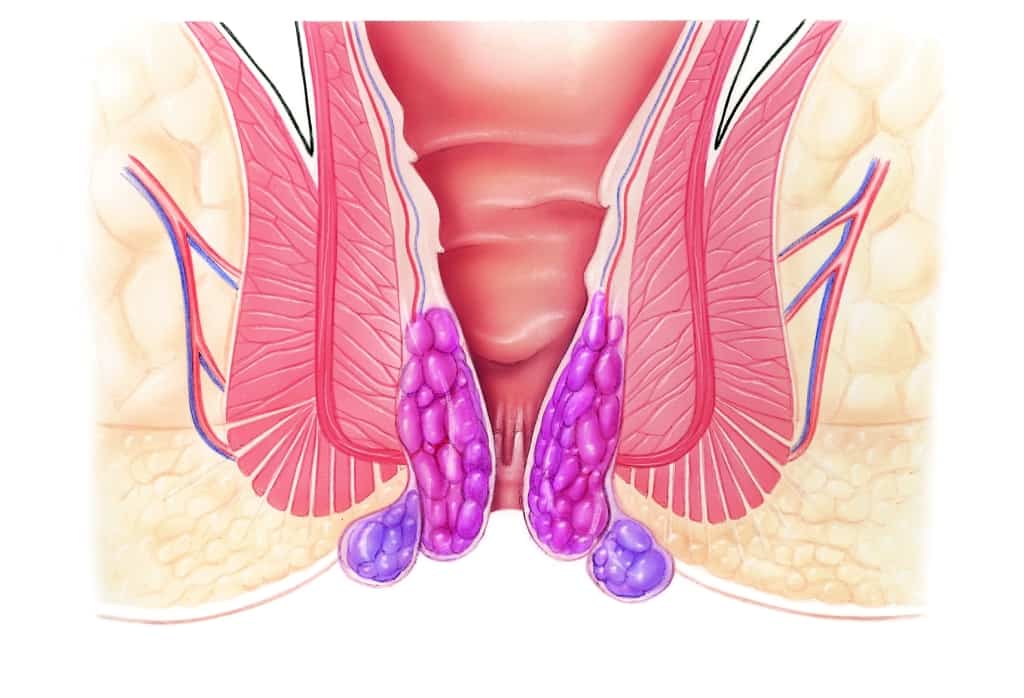
Subject to the stage of the hemorrhoidal disease, the following treatment options are carried out:
- sclerotherapy
- rubber band litigation
- Milligan-Morgan procedure
- stapled hemorrhoidopexy (Longo´s procedure)

Subject to the stage of the hemorrhoidal disease, the following treatment options are carried out:
Sclerotherapy (= shrinking blood vessels; may cause skin irritations) is a treatment for stage I-II of hemorrhoidal disease. During this procedure, we inject a sclerosing solution (e.g., Aethoxysklerol®) just above the hemorrhoids into the mucous membrane. This causes a scarring process that helps shrink and fix the hemorrhoids. Administered correctly, the low-risk sclerotherapy is painless. Main risk: a rare, slight bleeding after the procedure.
Rubber band litigation is a treatment for stage II (-III) of hemorrhoidal disease. During this painless procedure, we insert a specific applicator through the open proctoscope (tube) in order to stanch an area of the mucous membrane just above the hemorrhoid by using a rubber band. The treated part of the mucous membrane falls off together with the rubber band after a few days. This causes scarring that shrinks and fixes the hemorrhoids. Main risk: bleeding 2-3 days after the procedure.
For several decades, the Milligan-Morgan procedure has been established as standard surgical treatment of hemorrhoidal disease. We perform a slightly modified version of the Milligan-Morgan procedure to treat stage III-IV of hemorrhoidal disease (III: in case of single prolapsed hemorrhoids, outpatient treatment; IV: in case of several fixed prolapsed hemorrhoids, inpatient-treatment). It is undergone under general or regional spinal anesthesia.
Preparation: Please do not eat solid food at the evening before surgery and take a Bisacodyl® suppository; micro-enema on the day of surgery.
At the beginning of the Milligan-Morgan procedure, a rectal examination (inspection, feeling for anomalies with fingers) and rectoscopy/proctoscopy (inserting a rectoscope for better vision) are carried out under anesthesia. It is followed by disinfection, covering and the insertion of an anal spreader.
Local anesthesia with adrenalin is optional. It reduces the pain and bleeding during surgery.
Protecting the anal sphincter, the enlarged hemorrhoid is electrosurgically removed, and the supplying blood vessels are sutured. The wound inside the anal canal is not stitched up on purpose. The removed tissue undergoes a histological examination at a laboratory.
After controlling the results and stanching the blood, an lidocaine ointment is administered inside the anal canal.
Passing stool after the Milligan-Morgan procedure is possible without constraints. The anal region should be showered with lukewarm water afterwards. Subsequently, a gauze swab with a lidocaine-panthenol ointment is applied. Taking painkillers is necessary for 1 week.
It depends on your occupation and your condition how long it takes to resume work. Generally, it is about 1-3 weeks.
Stapled hemorrhoidopexy, also called Longo´s procedure, has been a standard procedure to treat prolapsed hemorrhoids of stage III of hemorrhoidal disease for many years.
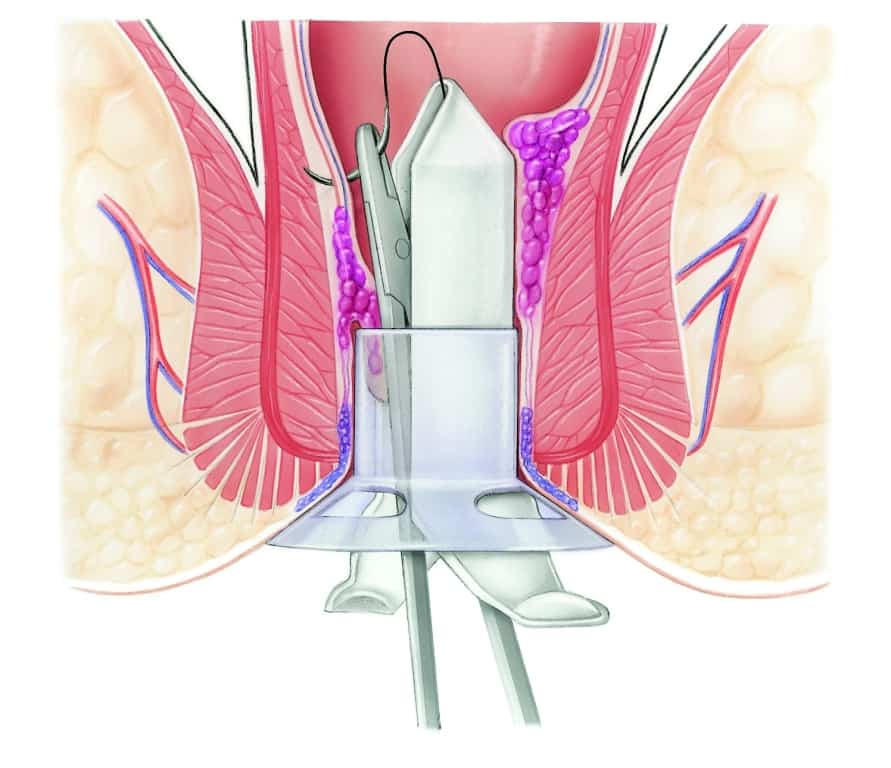
During stapled hemorrhoidopexy, a layer of mucous membrane is removed just above the hemorrhoid, using a circular stapler, and the wound is sutured with titanium staples. The lower rectum is “lifted”, and the flow of blood of hemorrhoid-supplying arteries is reduced.
Stapled hemorrhoidopexy needs the same preparations, anesthesia and examinations as the Milligan-Morgan procedure.
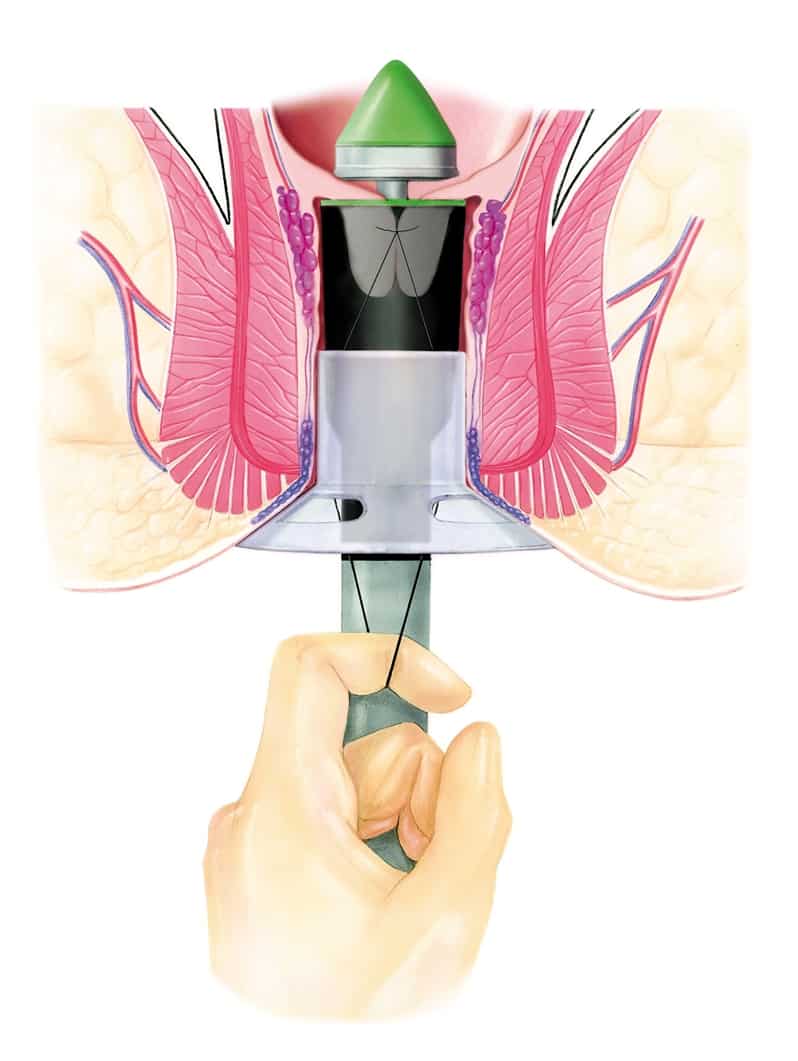
After disinfecting the skin, a special instrument ensures a circular suture above the hemorrhoid. This suture is crucial for the proper removal of the layer of mucous membrane as well as the stapler. Large hemorrhoids and a narrow anal canal make the procedure more difficult to carry out, which is why the surgeon´s experience and anatomical expertise is very important in order to success.
The layer of mucous membrane is then collected by the stapler. The stapler closes, and the wound is sutured within the same step, after controlling the correct position of the instrument.
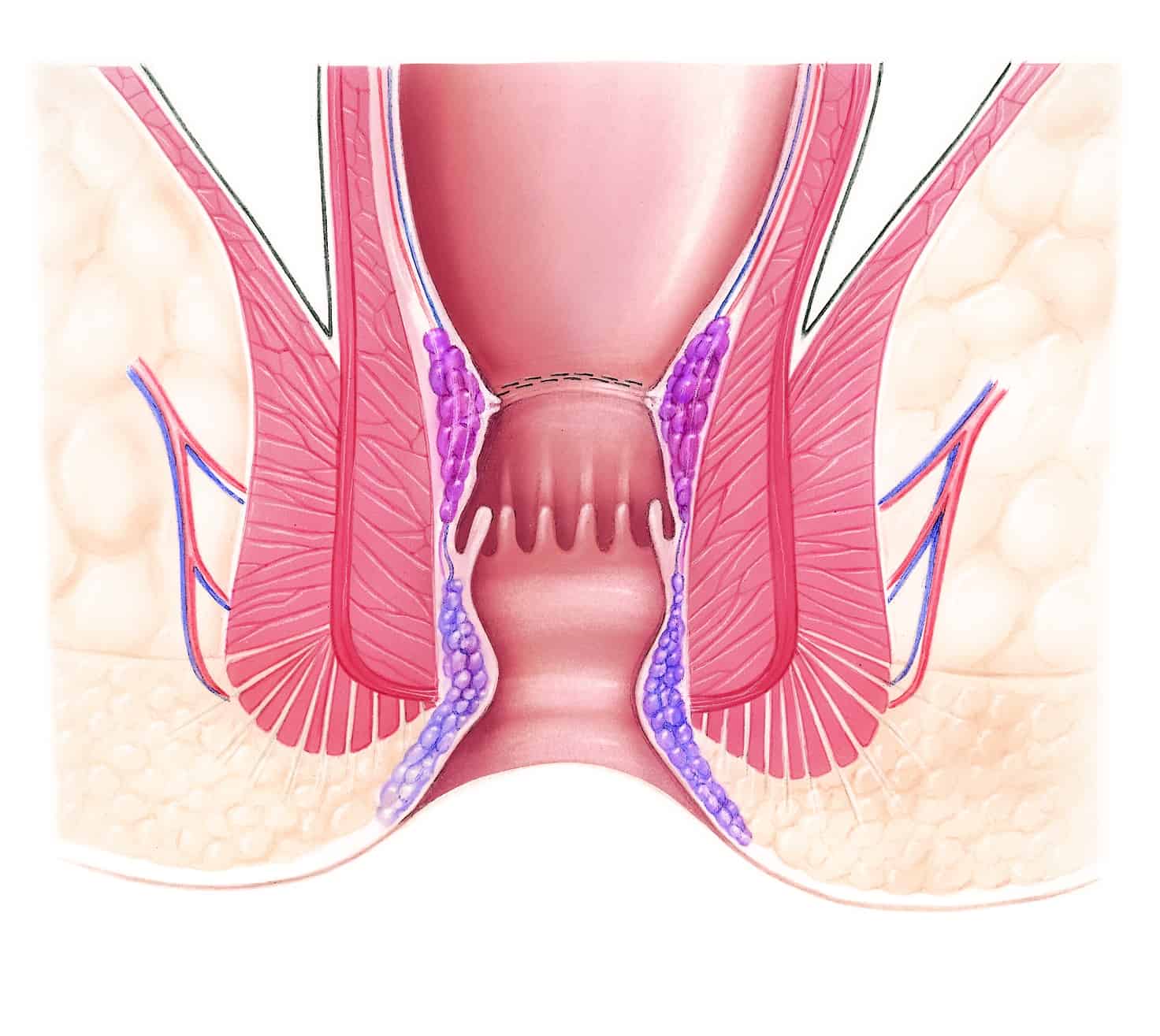
Given more than one hemorrhoid to treat, the advantage of the stapled hemorrhoidopexy is the lack of a wound within the sensitive anal canal because the suture is located within the non-sensitive area at the end of the rectum. This reduces the recovery period, and patients can quickly resume work. Some research papers point out the high recurrence rate, but it could not be verified within the patients of Beta Klinik (> 800). Problems in terms of fecal continence are very rare (< 0.5%).
Staying at least one night at the ward of Beta Klinik is necessary after the stapled hemorrhoidopexy in order to detect and stop potential bleedings (less than 1% of the patients at Beta Klinik). Painkillers are necessary the day of surgery and the day after it. Like Milligan-Morgan procedure, eating is possible on the day of surgery. Softening the stool and refraining from challenging physical activities is crucial for about 8-10 days.